
Complete the call-to-action survey!
Read more about the weekly call to action:
Sepsis remains the leading cause of hospitalization and hospital mortality, contributing to over a third of hospital deaths. Sepsis can be complex, difficult to identify, and often progresses rapidly, posing a significant challenge to clinicians and hospital quality improvement leaders. Tackling sepsis mortality can feel like a big task with many possible directions to take for improvement.
Join us in working toward reducing sepsis mortality one week at a time during our “call to action” email series.
Hospital Sepsis Program Core Elements
The development of a multi-disciplinary hospital sepsis program is critical to monitoring and improving the management and outcomes of patients with sepsis. Hospital quality improvement programs focused on sepsis have been associated with reductions in hospital mortality, length of stay, and healthcare costs. The Hospital Sepsis Program Core Elements include:
-
-
- Hospital Leadership Commitment: Dedicating the necessary human, financial, and information technology resources.
- Accountability: Appointing a leader or co-leaders responsible for program goals and outcomes.
- Multi-Professional Expertise: Engaging key partners throughout the hospital and healthcare system.
- Action: Implementing structures and processes to improve the identification of management of, and recovery from sepsis.
- Tracking: Measuring sepsis epidemiology, management, and outcomes to assess the impact of sepsis initiatives and progress toward program goals.
- Reporting: Providing information on sepsis management and outcomes to relevant partners.
- Education: Providing sepsis education to healthcare professionals, patients, and family/caregivers.
-
Additional Weekly Content
Click to expand for more information on each core element.
Week 1: Leadership, Accountability and Measuring Sepsis Outcomes
INTRODUCTION
The timely identification and treatment of sepsis is a major healthcare priority. Any type of infection can lead to sepsis and worldwide, one third of the people who develop sepsis will die. In fact, mortality from sepsis increases by as much as 7-9% every hour treatment is delayed.* Fortunately, sepsis deaths can be prevented. As many as 80% of sepsis deaths could be prevented with standardization and mobilization of tools and protocols that are already available.* A key aspect of successful implementation of a sepsis program is establishing a strong leadership commitment. Leaders must dedicate the necessary human, financial and technological resources to sepsis improvement programs. Further, an accountable leader must be responsible for establishing and working to achieve sepsis program goals. With a seemingly endless list of competing priorities, capturing leadership attention may seem difficult.
This week, we’ll focus on setting the stage for acting against sepsis. The Centers for Disease Control and Prevention (CDC) Sepsis Program Core elements of ‘leadership’ and ‘accountability’ correspond to this week’s activity.
*Source: Sepsis Alliance. Sepsis Fact Sheet. 2023. https://www.sepsis.org/education/resources/fact-sheets/
NATIONAL DATA
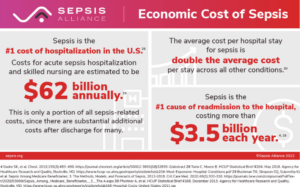
The costs associated with sepsis, both human and financial, are exorbitant. Costs for acute sepsis hospitalization and skilled nursing are estimated to be $62 billion annually. Review the Sepsis Alliance fact sheet to learn more.
IMPORTANT INFORMATION FOR SEPSIS IMPROVEMENT: The Sepsis Mortality Measure
How is sepsis defined? Communicating with leadership about what specifically your facility is trying to improve is essential to gaining buy-in. For the purposes of the Telligen HQIC program, we are aiming to improve the 30-day sepsis mortality rate. The denominator comprises hospitalized patients with a sepsis diagnosis and the numerator comprises patients with a death date less than or equal to 30 days after their latest sepsis diagnosis. There are currently no exclusions to this measure and is calculated using Medicare FFS claims data. Please review the Telligen Specifications Manual v6.0 for additional detail. You may also view our additional sepsis measures including post-operative sepsis mortality. You may also contact your quality improvement facilitator for additional support or reach out to HQICTeam@telligen.com with questions.
Visual representation of your facility’s data can support you in communicating that sepsis mortality is a major priority. Login to CDS at ahacds.org to view your facility’s unique run charts. Click here for an example of a run chart at the program level.
ADDITIONAL RESOURCES
- Sepsis Core Elements Webinar Series (Free CEs!) – Leadership Commitment and Accountability and Multi-Professional Expertise | CDC
- Hospital Sepsis Program Core Elements: Assessment Tool | CDC
- Sepsis Fact Sheets and Information Guides | Sepsis Alliance
- Publications detailing the costs of sepsis – Technical Resources & Guidelines | CDC
Week 2: Multi-Professional Experience and Action
INTRODUCTION
The primary goal of a hospital sepsis program is to improve treatment outcomes for patients. The approach to achieving positive patient outcomes and reducing sepsis mortality is multifaceted. Although the Centers for Disease Control and Prevention (CDC) recommends implementing a sepsis coordinator role for overseeing the implementation of day-to-day aspects of the sepsis program, impacting sepsis outcomes requires a multi-disciplinary team. Quality improvement leaders, clinicians across hospital domains, information technology team members, and patients and families must be able to provide input regarding sepsis program activities. Further, the actions of the sepsis program should be focused on leveraging evidence-based practices and technology to establish standardized screening processes, treatment guidelines and post-discharge care coordination.
There are a variety of evidence-based practices for sepsis care you may choose to implement at your facility, but where should you start? This week, we focus on getting the right people to the table and selecting interventions that will make an impact. The CDC’s Hospital Sepsis Program Core Elements of ‘multi-professional expertise’ and ‘action’ correspond to this week’s activity.
NATIONAL DATA
The Society of Critical Care Medicine Surviving Sepsis Campaign (SCC) guidelines for the early identification and treatment of patients with sepsis along with the development of the Centers for Medicare and Medicaid Services (CMS) SEP-1 measure have significantly impacted sepsis care in the U.S.
However, recent data collected from the National Healthcare Safety Network 2022 Annual Survey reveal that opportunity still exists in building robust hospital sepsis committees.*
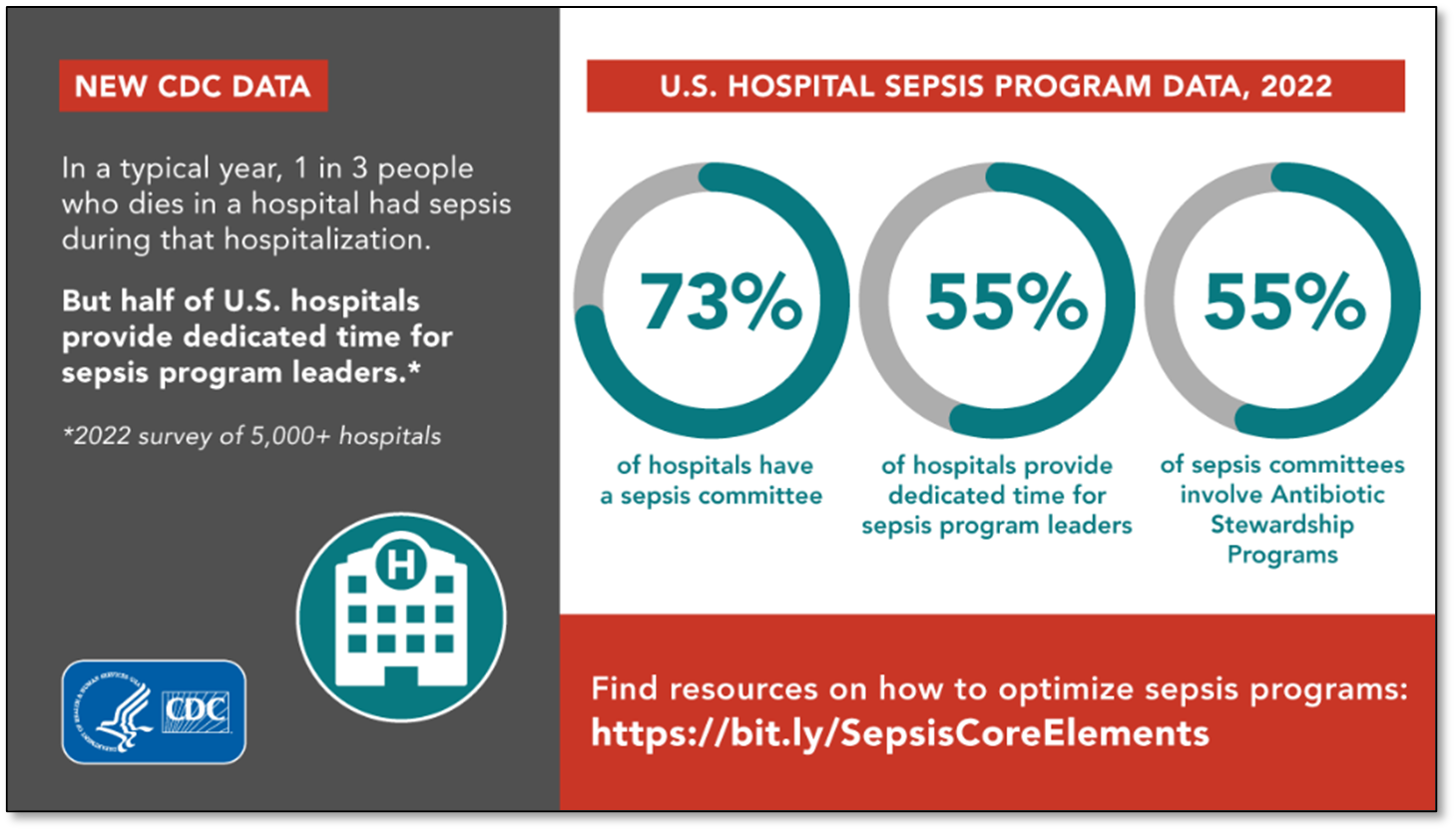
*CDC launches new effort aimed at strengthening survival and recovery rates for all sepsis patients
IMPORTANT INFORMATION FOR SEPSIS IMPROVEMENT: Evidence-Based Sepsis Guidelines
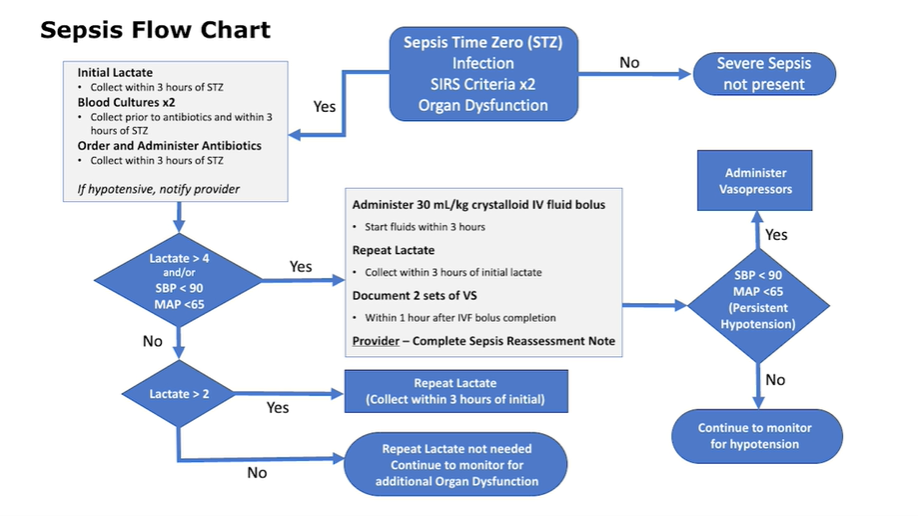
Hospital guidelines or standardized care pathways can greatly enhance the effectiveness of sepsis programs by establishing clear recommendations for care. Regardless of whether you report the SEP-1 measure to the Centers for Medicare and Medicaid Services (CMS) as part of IQR, reviewing the SEP-1 measure specifications may be useful in understanding the current standard of care for patients with sepsis. Further, you can review the Surviving Sepsis Campaign’s updated 2021 guidelines here for any recent changes to recommendations. In addition to reviewing guidelines from national organizations, it can be very helpful to refer to examples from peers. Please see below an example from Henry Ford Allegiance Health of a sepsis flow sheet featured on the CDC’s recent webinar, ‘Action: Hospital Sepsis Program Core Elements.’
- For additional ready-to-use resources, review the Hour-1 Bundle printouts and pocket cards from SCC.
- The CDC also provides additional screening tools and clinical pathway examples here.
- Click here for an example of a screening tool.
ADDITIONAL RESOURCES
- Sepsis Core Elements Webinar Series (Free CEs!) – Accountability and Multi-Professional Experience and Action | CDC
- Hospital Sepsis Program Core Elements: Assessment Tool | CDC
- Hospital Sepsis Program Core Elements | CDC
- Quality Improvement Principles to Improve the Care of Patients with Severe Sepsis | NIH
- Toolkit for Using AHRQ Quality Indicators for Sepsis | AHRQ
Week 3: Tracking, Reporting, Health Equity and Social Determinants of Health
INTRODUCTION
Tracking sepsis events, timely care interventions and associated patient outcomes are critical to understanding how sepsis is managed in your facility. Improving your understanding of trends, gaps in care and progress toward sepsis goals will aid you in prioritizing improvement activities. Effective recognition and treatment of sepsis is multidisciplinary and multifaceted. Furthermore, equity, social determinants of health and rural considerations may influence sepsis outcomes. Time and resources may be limited which can make it unrealistic to measure everything sepsis-related all the time.
This week, we will focus on prioritizing what to track and strategies for reporting your findings to staff and improvement teams. The Centers for Disease Control and Prevention (CDC) Hospital Sepsis Program Core Elements of ‘tracking’ and ‘reporting’ correspond to this week’s activity.
NATIONAL DATA
CMS’s Severe Sepsis and Septic Shock Management Bundle (SEP-1) and More
The SEP-1 bundle elements and/or the American College of Emergency Physicians (ACEP) sepsis quality metrics are a great place to start when thinking about tracking sepsis improvement activities. A recent study evaluated rural and urban hospital performance on each of the bundle elements. The study found that rural facilities achieved higher SEP-1 bundle compliance than urban centers. View the table below to see how rural and urban facilities compare for completing each ACEP measure.
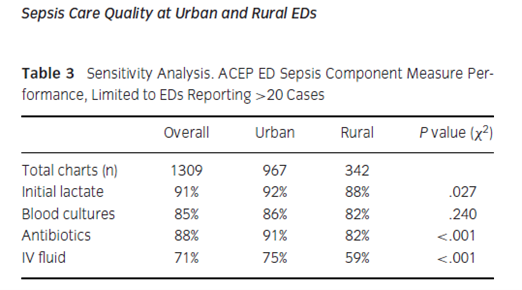
Click to expand. (Greenwood-Ericksen et al., 2019)
This is just one example of elements you might track. Be sure to keep in mind the unique priorities of your facility. Consider other aspects of sepsis improvement that may take tracking priority.
CASE STUDY
Track and Report Out Sepsis Data
After you’ve made an effort to track one or more elements of your facility’s sepsis performance, it is critical to report out this information to staff and improvement teams so that you may dialogue about opportunities to improve. This case study required clinicians to attest to completion of bundle elements within the EHR. See section “Accountability and Driving Resilient Care Redesign.” Your staff or leader report out may include:
-
- Unit level data
- Trends over time (login to CDS to view your sepsis mortality data)
- Comparative data (Contact your HQIC quality improvement facilitator for this information)
- Clinician feedback
ADDITIONAL RESOURCES
-
- Hospital Sepsis Program Core Elements | CDC
- Sepsis Alliance Institute – Create a free account to access to tools and templates.
- Multi Language Resources | Sepsis Alliance
- Hospital Toolkit for Adult Sepsis Surveillance | CDC
- Sepsis Core Elements Webinar Series (Free CEs!) | CDC
Week 4: Education
INTRODUCTION
For optimal sepsis treatment and outcomes, it is imperative that hospital staff have strong knowledge of sepsis and understand their role in team-based management of sepsis. Educational efforts should be focused on all healthcare workers involved in sepsis care, all patient-facing staff and all health profession trainees. There are many methods of providing education to hospital staff, including simulation or case-based training, in-person or video-recorded lectures, flyers or posters and email newsletters. The optimal approach to education may vary by audience.
This week, we will focus on developing staff education programs as well as strategies for educating patients, families and caregivers. The Centers for Disease Control and Prevention (CDC) Sepsis Program Core Element of ‘Education’ corresponds to this week’s activity.
NATIONAL DATA
Many patients diagnosed with sepsis suffer from post-sepsis syndrome. Post-sepsis syndrome is defined as a constellation of long-term physical, medical, cognitive and psychological issues follow sepsis recovery. It is estimated that around 75% of sepsis survivors develop at least one new medical, psychological or cognitive diagnosis after hospital discharge. Early detection and treatment are essential for survival and limiting disability for survivors. You can find additional information on post-sepsis syndrome here.
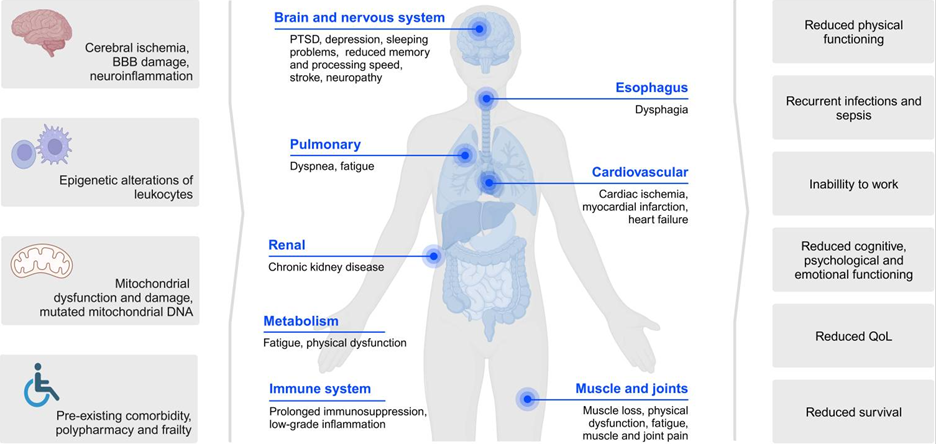
Click to Expand. (van der Slikke et al., 2023)
IMPORTANT INFORMATION FOR SEPSIS EDUCATION – When Should You Educate?
Knowledge of sepsis is also important for patients, families and caregivers. Patients hospitalized for sepsis are at increased risk for subsequent episodes of sepsis. Hospitalization and post-hospital follow-up are excellent opportunities to educate patients, families and caregivers! Despite the increased risk for recurrent sepsis, many patients are unaware of both their diagnosis of sepsis and their risk for recurrent sepsis. In fact, many sepsis survivors are dissatisfied with sepsis education. The Surviving Sepsis Campaign guidelines suggest offering both verbal and written sepsis education prior to hospital discharge and in the follow-up setting. Education may facilitate timely health-seeking behavior in sepsis survivors who experience complications.
Key elements of sepsis education for patients, families and caregivers include:
-
- Signs and symptoms of sepsis
- When to suspect sepsis
- When and where to seek evaluation for potential sepsis
- Infection prevention measures that should be followed post-discharge
- Referrals to treat patients with post-sepsis syndrome, including the physical and psychological long-term effects
- When, where and the importance of their follow up with a primary care provider following hospital discharge
ADDITIONAL RESOURCES
-
- Sepsis Education Page – Patients, Families, Caregivers and Health Professionals | CDC
- Sepsis Core Elements Webinar Series (Free CEs!) – Education | CDC
- Post-Sepsis Syndrome Video for Patients – Life After Sepsis | Sepsis Alliance
- Multi-language Resources | Sepsis Alliance
- Life After Sepsis Fact Sheet | CDC
- Sepsis Alliance Institute: Free Educational Webinars
- Upcoming Events in December | Sepsis Alliance
- Hospital Sepsis Program Core Elements Assessment Tool | CDC
Week 5: Patient and Family Engagement and Older Adult Considerations
INTRODUCTION
This week, we will be focusing on sepsis and elderly care considerations and patient and family engagement (PFE). Older adults are at a higher risk of developing infections due to having a weakened immune system and chronic health conditions like diabetes, heart and lung diseases. These comorbidities can increase the risk of developing infections that can transform into sepsis. It is important to be aware that the older adult may not present with “normal” symptoms like fever; confusion and tiredness are major signs of sepsis for older adults. Adults aged 65 years and older are 13 times more likely to be hospitalized with sepsis than adults younger than 65. 63% of older adults 60 years and older that are admitted to the ICU present with sepsis upon admission. The Sepsis Alliance has provided opportunities for families and healthcare providers to have awareness of considerations when caring for the older population.
This week, we will consider sepsis and aging and develop a plan for engaging patients and families in sepsis mortality prevention.
NATIONAL DATA
Research shows that elderly patients are much more likely to suffer lasting consequences from sepsis. In addition to amputation and organ failure, which are common outcomes for any sepsis survivor, older patients can suffer major cognitive and physical limitations.
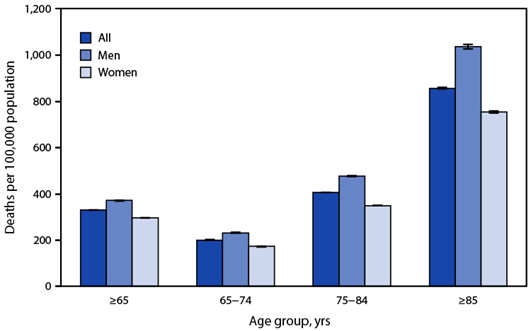
Sepsis-Related* Death Rates† Among Persons Aged ≥65 Years, by Age Group and Sex — National Vital Statistics System, United States, 2021
In 2021, the sepsis-related death rate among persons aged ≥65 years was 330.9 deaths per 100,000 population. The rate among men (371.7) was higher than that among women (297.4).
Sepsis-related death rates among men were higher than those among women in each age group: 232.7 versus 173.0 (65–74 years), 477.3 versus 349.8 (75–84 years), and 1,037.8 versus 755.5 (≥85 years).
Sepsis-related death rates increased with age from 201.1 among persons aged 65–74 years to 858.3 among those aged ≥85 years. Sepsis-related death rates increased with age among both men and women.
Source: National Center for Health Statistics, National Vital Statistics System, Mortality Data, 2021. https://blogs.cdc.gov/nchs/2023/09/22/7456/
IMPORTANT INFORMATION FOR SEPSIS CARE IN OLDER ADULTS
The Sepsis Alliance has gathered critical information on detecting sepsis in the elderly, data and what to do if there is a concern of sepsis. Learn more with this Sepsis Fact Sheet.
{kind=link}
 Sepsis and Aging Information Guide
Sepsis and Aging Information Guide
PATIENT AND FAMILY ENGAGEMENT
Research has shown that when patients and families are included in the healthcare plan, it can lead to improvement in patient safety and quality of care. The Agency for Healthcare Research and Quality (AHRQ) has created a guide that promotes patient and family engagement in safety and quality of care during hospitalization.
Patients and families play several key roles in improving the safety and outcomes of their own care. These include accessing information that helps in determining the correct diagnosis, involving themselves in decisions about appropriate care, choosing an appropriate provider, following the agreed-upon treatment plan, and speaking up when something does not go as expected or appears to be a medical error. Healthcare organizations and clinicians have a responsibility to encourage and enable patients and families to become proactively engaged in these activities.
An extensive literature review demonstrates the association between active engagement of patients at all stages of care – from diagnosis to treatment – and a variety of important outcomes. Patient engagement can take various forms including:
-
- Participation in diagnosis. Accurate diagnosis requires that the patient and/or their representative provide the full story of health issues.
- Shared decision making. Appropriate decisions about treatment must be based on both clinical evidence and patient preferences, values and circumstances.
- Following the treatment plan. Discuss with the patient and family the importance of following a health plan and where the patient is at with compliance.
- Another pair of eyes. Including the patient and family with their care, who know the patient well, will be able to provide information when the patient is not at baseline.
ADDITIONAL RESOURCES
Week 6: Emergency Department and Emergency Medical Services Collaboration
INTRODUCTION
Emergency Medical Services (EMS) play a major role in the diagnosis and early management of patients with severe sepsis. In fact, EMS personnel frequently represent the first medical contact for sepsis patients. As many as 87% of sepsis cases start in the community prior to hospitalization. Rapid response to sepsis by EMS personnel may expedite lifesaving care when the patient reaches the emergency department (ED). For this reason, collaboration amongst local EMS and hospital EDs is essential to sepsis identification and treatment.
This week, we will discuss methods for engaging EMS in sepsis improvement work.
CASE STUDY: Sepsis and EMS Survey
This case study reviews a 2019 survey conducted by the Sepsis Alliance and the National Association of Emergency Medical Technicians (NAEMT). Key findings include that only half of EMS practitioners are very confident in their ability to recognize the signs and symptoms of sepsis.
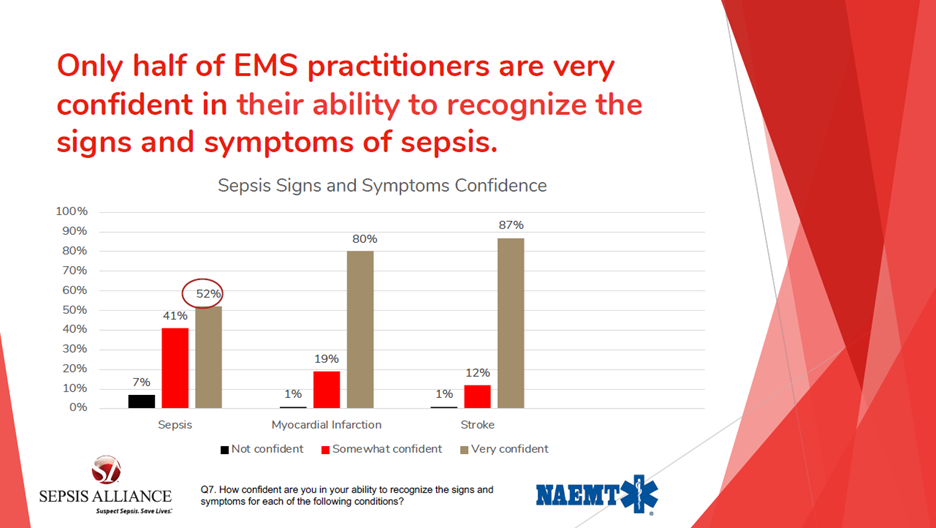
Source: Sepsis and EMS Survey | Sepsis Alliance
IMPORTANT INFORMATION FOR COLLABORATING WITH EMS
Collaborating across hospital locations is a key aspect of improving the quality of sepsis care. Leaders and clinicians in the inpatient, ICU and ED settings should be fully engaged in hospital sepsis program activities. Facility-wide participation is important to ensure coordination of sepsis care throughout the hospital. EMS personnel are routinely involved in patient care preceding hospital arrival; thus, they are important members of the sepsis care team. Be sure to include EMS in your improvement efforts! Below are some strategies for keeping EMS in the loop:
-
- Engage EMS leaders in sepsis committee meetings. Even volunteer departments have leadership teams who can be engaged in sepsis quality improvement.
- Collaborate on existing protocols. Meet with EMS leaders and clinicians to discuss their current sepsis protocols. Work together to identify gaps in care and opportunities to improve communication and align policies with hospital protocol. Protocols to discuss include sepsis screening, intervention, hand-off communication and documentation. You may consider reviewing the 2022 Actionable Patient Safety Solutions Performance Improvement Plan (page 9).
- Provide sepsis resources to EMS leaders. Collaborate to develop pocket cards, posters, stickers or badge cards to prompt EMS personnel to consider sepsis and identify transfer and treatment next steps. Continuing education for EMS personnel regarding sepsis can be found here.
ADDITIONAL RESOURCES
Actions to Take TODAY!
Click to expand for the weekly call to action and survey.
Week 1: Start the Sepsis Conversation with Hospital Leadership
Informing leadership of the current state of sepsis improvement work is an important aspect of engagement. Leaders are unable to support sepsis work financially and administratively if they are unaware of the impact sepsis has on patient outcomes and hospital finances. It is the accountable sepsis leader’s responsibility to inform facility leaders at all levels. This may include, but is not limited to the board of directors, medical director, CEO and CNO. This week’s activity serves as a starting point for communicating with leaders about sepsis.
This activity is intended to be completed within one week of November 9. Follow the step-by-step instructions below.
- The accountable sepsis improvement leader(s) (i.e., quality director, physician, nurse) approach the CEO to request focused sepsis discussion time at an upcoming board of directors meeting. Download this letter template.
- Clinical leaders collect relevant information to present to the board including, but not limited to:
- Sepsis mortality data and run chart from CDS (login and download at ahacds.org).
- Current sepsis improvement activities including clinical tools and policies.
- At least one improvement goal related to sepsis. Use SMART goal formatting found on page 7 of the Quality Improvement Workbook.
- Gaps in current programming and proposal for what is needed.
- Invite board of directors to engage in discussion with the clinical improvement team and propose a schedule for regular report out (i.e., quarterly) of sepsis improvement challenges, success stories and activities.
*Note: These activities are not intended to guide clinical decision making and are for quality improvement purposes only.
TAKE THE WEEKLY SURVEY!
Answer just 2 questions to generate your certificate of completion.
Week 2: Review Sepsis Policies and Procedures
To address the “multi-professional expertise’ and ‘action’ core elements, start by reviewing your sepsis policies and procedures and identify at least one aspect of your policy that you can edit and improve. You may also choose to share your proposed edits with your improvement team for feedback. This week’s activity serves as a starting point for engaging multi-disciplinary team members and developing interventions that are effective for your facility’s unique characteristics.
This activity is intended to be completed within one week of November 16. Follow the step-by-step instructions below.
1. As the quality leader, review your current sepsis committee team charter (or create one using a team charter template found on page 12 of the Quality Improvement Workbook) and ensure representation from one or more of the following departments:
a. Emergency Department
b. Inpatient/ICU
c. Antibiotic Stewardship Committee/Pharmacy
d. Infectious Disease
e. Information Technology
f. Social Work/Case Management
g. EMS representative
If you are missing one or more of these representatives, choose one to reach out to and encourage them to attend your next committee meeting. If you are in the process of getting your committee organized, write down the names of individuals from these departments you can contact who may be willing to be a part of the team.
2. Review your current sepsis policies and procedures and choose ONE area to put on the agenda for discussion at your next committee meeting. Examples include:
a. Screening
b. Clinical evaluation
c. Diagnosis
d. Antimicrobial selection
e. Source control
f. Fluid resuscitation
g. Indications for treatment escalation
h. Antimicrobial narrowing and stopping
i. Patient and family/caregiver education
j. Peri-discharge management
Follow-up Actions (these may take longer than one week):
3. After you’ve made your selection, plan to brainstorm with your committee on ONE action you can take to improve the policy or process related to your above selection. Determine who and what needs to be involved, then implement your change. This can be a small test of change – challenge yourself to keep it simple. You may use the PDSA worksheet to help you plan. Be sure to include how you will notify staff of your proposed change and set a time to meet with your team or check on the intervention again in one month to adapt, adopt or abandon the change.
4. Submit any policy or process revisions found via your PDSA for approval by leadership and medical staff during the next review period.
*Note: These activities are not intended to guide clinical decision making and are for quality improvement purposes only.
TAKE THE WEEKLY SURVEY!
Answer just 2 questions to generate your certificate of completion.
Week 3: Sepsis Chart Review
This activity is intended to be completed within one week of November 30. Follow the step-by-step instructions below.
1. Complete the bundle compliance feedback form for at least three recent sepsis cases. *Note: This is just one way to review cases. If you already have a method built into your EHR or a root cause analysis process, you may use that.
2. Analyze the cases to identify any similarities or significant differences between them.
3. Answer the reflection questions below independently or with your improvement team:
-
-
- What opportunities for improvement were identified following case review?
- Who will you share your findings with? You may choose to send feedback forms to providers with a brief note explaining why. Download an example here.
*Note: These activities are not intended to guide clinical decision making and are for quality improvement purposes only.
TAKE THE WEEKLY SURVEY!
Answer just 2 questions to generate your certificate of completion.
-
Week 4: Spread the Word About Sepsis
This week’s activity serves as a starting point for gathering educational tools and developing a plan for routinely educating all staff, patients, families and caregivers. This activity is intended to be completed within one week of December 5. Follow the step-by-step instructions below.
- Create a free member account with the Sepsis Alliance to access several educational materials for providers and patients. Review and save materials that are relevant to your facility.
- Select at least one poster or fact sheet from either the CDC or Sepsis Alliance to print and make available in prominent areas for clinical staff and patient access. Or you can order free “Get Ahead of Sepsis” materials in English and Spanish (brochures, fact sheets, posters, pocket guide, videos) from the CDC in two ways:
- Visit CDC Publications On Demand, select “Sepsis” from the Programs drop-down menu and click “Apply.”
- Call 1-800-CDC-INFO.
- Schedule a day and time to attend nursing staff shift huddle (ED and Inpatient) to review the sepsis education materials you printed, including how and when to share the information with patients (i.e., at discharge).
*Note: These activities are not intended to guide clinical decision making and are for quality improvement purposes only.
TAKE THE WEEKLY SURVEY!
Answer just 2 questions to generate your certificate of completion.
Week 5: Provide Education to Your Patient and Family Engagement Advisory Council (PFAC)
This activity is intended to be completed within one week of December 14. Follow the step-by-step instructions below.
- Provide the Get Ahead of Sepsis flyer to your Patient and Family Engagement Committee or Advisory Council.
- Ask your PFAC to participate in a discussion about how the hospital or unit(s) may be able to use the flyer and/or how to incorporate sepsis education into existing workflows? This discussion can take place in person, on zoom, or via email.
- After collecting responses from the PFAC, what opportunities for improvement were identified following the review of educational materials?
*Note: These activities are not intended to guide clinical decision making and are for quality improvement purposes only.
TAKE THE WEEKLY SURVEY!
Answer just 2 questions to generate your certificate of completion.
Week 6: Connect with Local EMS
This week’s activity serves as a starting point for collaborating with EMS to align pre-hospital and hospital identification and treatment protocols.
- Review the Sepsis: First Response 15-minute educational video and results of the EMS Case Study Survey included in this week’s content to familiarize yourself with the EMS approach to sepsis care.
- As the quality improvement leader, connect with your local EMS leaders by phone or email to share the hospital’s sepsis protocols and request a meeting to look for opportunities for collaboration and alignment between hospital and EMS protocols. As an alternative, invite an EMS representative to your next sepsis committee meeting.
- During your meeting preparation, consider overlapping gaps between hospitals and EMS identified in sepsis prevention recognition and treatment as outlined by the 2022 Actionable Patient Safety Solutions Performance Improvement Plan for the Early Detection and Treatment of Sepsis (page 11).
*Note: These activities are not intended to guide clinical decision making and are for quality improvement purposes only.
TAKE THE WEEKLY SURVEY!
Answer just 2 questions to generate your certificate of completion.
Access additional tools and resources at Telligen’s Hospital Resource Page.
Who We Help

nursing homes

clinicians
hospitals
