
Health Equity
Your one-stop shop for health equity resources.
Health Equity
Your one-stop shop for health equity resources.
Health equity is the state in which everyone has a fair and just opportunity to attain their highest level of health. Achieving this requires focused and ongoing societal efforts to address historical and contemporary injustices; overcome economic, social and other obstacles to health and healthcare; and eliminate preventable health disparities.
Demonstrate your commitment to making health equity a priority in your organization or community by exploring the resources below!

Health Literacy
According to Healthy People 2030, personal health literacy is the degree to which individuals have the ability to find, understand, and use information and services to inform health-related decisions and actions for themselves and others. Organizational health literacy is the degree to which organizations equitably enable individuals to find, understand, and use information and services to inform health-related decisions and actions for themselves and others.
Low health literacy is associated with reduced use of preventive services, poorly managed chronic conditions, higher mortality, medication errors, misdiagnoses due to poor communication between providers and patients, low rates of treatment compliance, hospital readmissions, unnecessary emergency room visits, longer hospital stays, fragmented access to care and poor responsiveness to public health emergencies.
Health Literacy Basics
- Center for Disease Control and Prevention (CDC) Health Literacy Basics
- Agency for Healthcare Research and Quality (AHRQ) Health Literacy
- Health Literacy in Healthy People 2030
- National Library of Medicine Health Literacy
- Center for Health Care Strategies Fact Sheets: Health Literacy
- CDC Health Literacy Website
- National Action Plan to Improve Health Literacy
- International Organization for Migration (IOM) Roundtable on Health Literacy
Tools for Providers
- CMS Improving the Collection of Social Determinants of Health Data with Z Codes
- AHRQ Health Literacy Universal Precautions Toolkit, 2nd Edition
- AHRQ Re-Engineered Discharge (RED) Toolkit
- AHRQ Teach-Back: Intervention
- Institute for Healthcare Improvement (IHI) Ask Me 3: Good Questions for Your Good Health
- AHRQ The SHARE Approach
Connecting the Dots: Health Equity & Health Literacy
(Printable flyer with state-specific data)
Tools for Patients and Families
- National Institute on Aging (NIA) Discussing Health Decisions with Your Doctor
- 12 Questions to Ask About Your Medicines
- AHRQ Provider Question Builder App
- NIH Office of Dietary Supplements My Dietary Supplement and Medicine Record
- NIH National Library of Medicine MedlinePlus: Understanding Medical Words
- NIH National Library of Medicine MedlinePlus: Some Common Abbreviations
- NIH National Library of Medicine MedlinePlus: Word Parts and What They Mean
Literacy Skills Assessment
Plain Language
- CDC Plain Language Materials and Resources
- The Federal Plain Language Action and Information Network (PLAIN) Language Guidelines
- Centers for Medicare & Medicaid Services (CMS) Guidelines for Effective Writing
- Center for Plain Language
- National Institute of Health (NIH) Clear Communication
- General Services Administration (GSA) Plain Language
- CDC Clear Communication Index Widget
- CDC Everyday Words for Public Health Communication
- CDC Are You Communicating Effectively with Older Adults?

Culturally and Linguistically Appropriate Services (CLAS)
The National CLAS Standards describe a framework to deliver services that are culturally and linguistically appropriate and respectful, and that respond to patients’ cultural health beliefs, preferences and communication needs. Standards can be employed by all members of a healthcare organization, state or community. In 2013, the U.S. Department of Health and Human Services Office released the enhanced National CLAS Standards to guide health and healthcare organizations in their efforts to ensure health equity.
CLAS Implementation Guide
A Practical Guide to Implementing the National CLAS Standards: For Racial, Ethnic and Linguistic Minorities, People with Disabilities and Sexual and Gender Minorities by the Centers for Medicare & Medicaid Services.
Behavioral Health Implementation Guide for CLAS
The Behavioral Health Guide is a companion document to the Blueprint for Advancing and Sustaining CLAS Policy and Practice. Together these documents provide concrete, feasible implementation strategies for the health and behavioral healthcare community to improve the provision of services to all individuals, regardless of race, ethnicity, language, socioeconomic status, and other cultural characteristics. The implementation examples are past grantee examples.
The Behavioral Health Guide is organized by the overarching themes of the 15 standards: Principal Standard;
Governance, Leadership and Workforce; Communication and Language Assistance; and Engagement, Continuous Improvement, and Accountability. Download the guide.
Watch the Advancing Behavioral Health Equity: National CLAS Standards in Action Webinar:
Health Equity Assessment
Use Telligen’s Health Equity Assessment to identify gaps and opportunities to improve health literacy and culturally appropriate health information and services.
Office of Minority Health Newsletters
The Office of Minority Health has launched a newsletter dedicated to raising awareness of culturally and linguistically appropriate services (CLAS) in health and healthcare. Learn how you can advance health equity through CLAS by reading the newsletters today.

Tools and Trainings to Advance Health Equity
Explore training opportunities, data resources, interventions and more.
Training Opportunities
- Telligen Trainings in the Secure Portal
- Centers for Disease Control and Prevention (CDC) Foundation’s Health Equity Video Series
- The opportunity to live our healthiest life includes our physical, mental, emotional and social wellbeing and is impacted by our community relationships. This video series highlights the importance of community-first approaches to public health and expanding the conversation on health equity.
- Centers for Medicare & Medicaid Services (CMS)
- Training From Other National Organizations
Interventions
Tools for Communities, Patients and Families
Data Resources
Tools for Providers
- CMS Disparities Impact Statement
- CMS Framework for Advancing Health Care in Rural, Tribal, and Geographically Isolated Communities
- CMS Guide to Developing a Language Access Plan
- CMS Providing Language Services to Diverse Populations: Lessons from the Field
- IHI Achieving Health Equity: A Guide for Health Care Organizations
- IHI How to Reduce Implicit Bias
- Harvard University – Project Implicit
Connecting the Dots: Health Equity & Health Literacy
(Printable flyer with state-specific data)
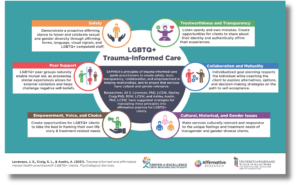
LGBTQ+ Resources
Check out the Center of Excellence LGBTQ+ Behavioral Health Equity resource page for videos, inforgraphics and more.
Download the LGBTQ+ Trauma-Informed Care Infographic.

Social Drivers of Health (SDOH)
According to Healthy People 2030, social determinants of health (SDOH) are the conditions in the environments where people are born, live, learn, work, play, worship and age that affect a wide range of health, functioning and quality-of-life outcomes and risks.
Social determinants (or drivers) of health in seniors may include income, health literacy, better quality food, housing, transportation, healthcare, social interactions and rural health.
Data Collection Tools
Improving the Collection of Social Determinants of Health (SDOH) Data with ICD-10-CM Z Codes
- Physicians can include supplemental ICD-10 “Z” codes in the patient’s diagnosis section and problem list, such as codes Z55–Z65, “Persons with potential health hazards related to socioeconomic and psychosocial circumstances.” Although Z codes are not generally reimbursable, including these codes in the medical record can help with population health, panel management, and quality improvement initiatives.15 Data collected may also eventually factor into value-based payment systems that will reimburse family physicians for this critical work to improve health. The data can also be useful in developing innovative solutions and partnerships to address the social driver that most directly affect a population. For example, Community of Hope created partnerships with a mobile farmer’s market as well as a bike-share program to promote healthy eating and exercise not only to the health center patients but also to the community in which the clinic is located.
Several screening instruments can aid physicians in identifying social drivers of health in a primary care setting:
- The National Association of Community Health Centers’ Protocol for Responding to and Assessing Patients’ Assets, Risks, and Experiences tool (PRAPARE) includes 15 core questions and five supplemental questions. The data can be directly uploaded into many electronic health records as structured data. It is generally administered by clinical or nonclinical staff at the time of the visit, but a paper version can be given to the patient to self-administer.
- The American Academy of Family Physicians offers a social needs screening tool, available in short- and long-form in English and Spanish, as part of The EveryONE Project. The short-form includes 11 questions and can be self-administered or administered by clinical or nonclinical staff.
- The Centers for Medicare & Medicaid Services Accountable Health Communities’ 10-question Health-Related Social Needs Screening Tool (AHC-HRSN) is meant to be self-administered.
Rather than expecting physicians to add “just one more thing” to their daily practice flow, social determinants screening and follow up must not be the sole responsibility of the physician but rather a team-based effort integrated into the practice’s care management workflows.
Adapted from “A Practical Approach to Screening for Social Determinants of Health.”


Focus on Rural Health
The factors driving rural health disparities vary widely. According to County Health Rankings, rural counties have higher premature death rates and rank lowest nationally in overall health outcomes. Telligen is supporting the efforts of rural communities across our four states – Colorado, Iowa, Illinois and Oklahoma – to develop local and regional solutions to advance health equity.
Browse resources, research and emerging insights into the many factors that shape rural opportunity, health and advance health equity.
Rural Health Resources
- Advancing Health Equity in Rural America (2 minute read)
- American Hospital Association Rural (AHA) Tools and Resources
- Centers for Disease Control and Prevention (CDC) – Rural Health
- Centers for Medicare & Medicaid Services Rural Health Resources
- County Health Rankings & Roadmaps
- Evidence-Based Toolkits for Rural Community Health
- Federal Office of Rural Health Policy (FORHP)
- National Rural Health Association
- Rural Health Information Hub – RHIhub
- What Works? Stategies to Improve Rural Health
Visit our calendar of events for health equity learning opportunities.
Contact Belinda Rogers or Temaka Williams to learn more about Telligen’s health equity initiatives.
Who We Help

nursing homes

clinicians
hospitals
